
Ultrasound can be very useful for assessing the small intestine. Ultrasound examination can provide information regarding bowel thickness, layering pattern, motility and evidence of diffuse or segmental dilation. The exam can be performed in dorsal or lateral recumbency. High frequency or linear probes offer the best resolution for assessing layering of bowel. In this blog, we will focus on assessing layering of small bowel.
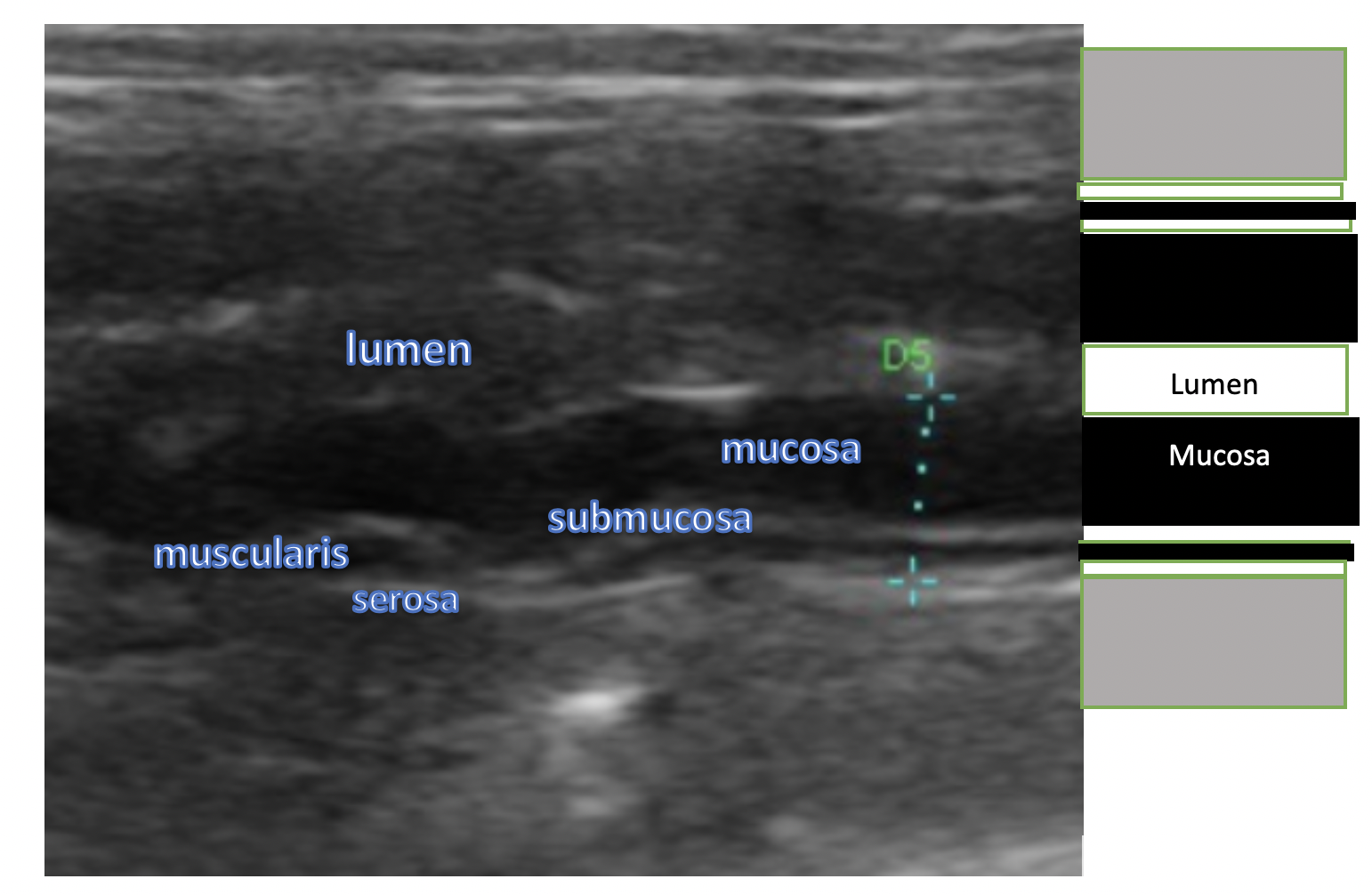
The ultrasonographic layers of the small bowel as noted below. Starting from the lumen of the bowel, the layers are 1) luminal-mucosal interface (bright), 2) mucosa (dark), 3) submucosa (bright), 4) muscularis (dark), and 5) serosa (bright):
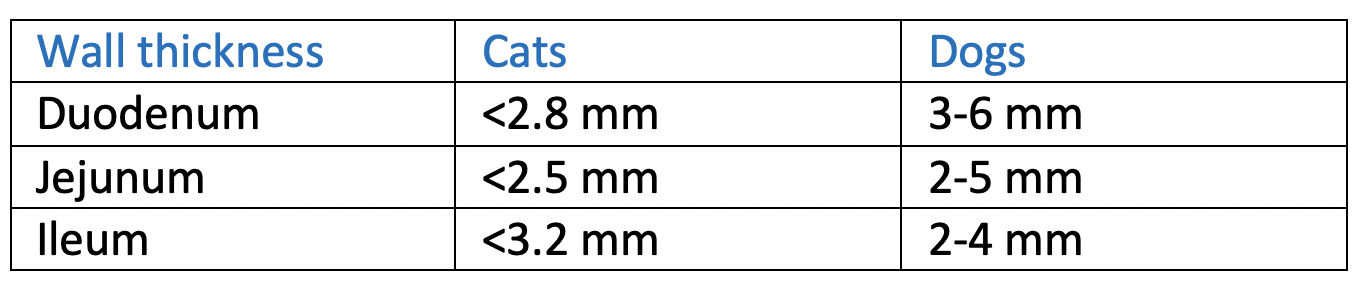
Normal wall thickness is generally as follows:
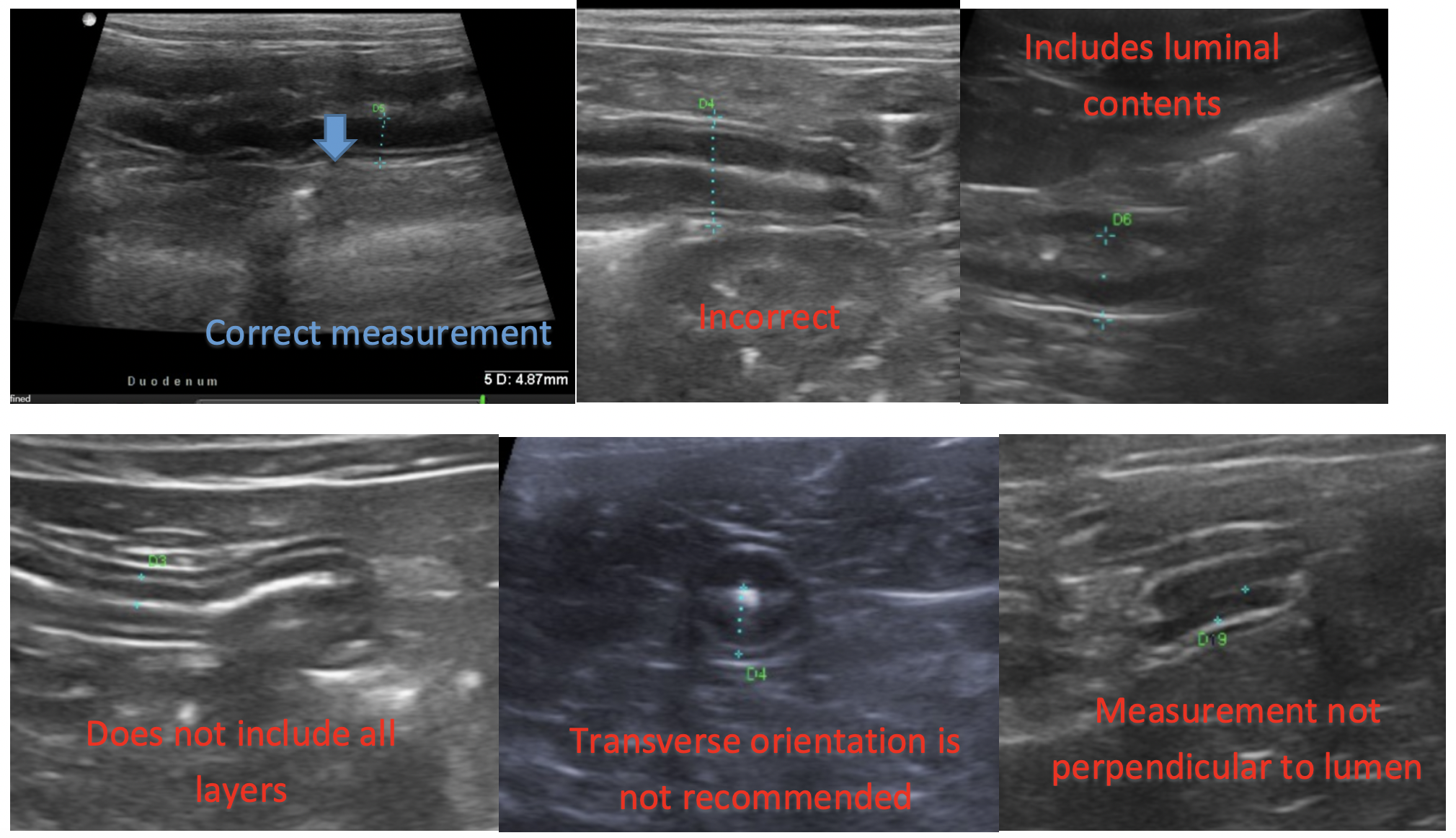
It is best to measure small bowel in long axis or longitudinal orientation rather than short axis or transverse orientation since you want to be perpendicular to the lumen and this cannot be assessed accurately in transverse views. I usually measure from the luminal/mucosal interface to the serosa to avoid including luminal contents in the measurements.
It is important to note that absence of ultrasonographic changes does not rule out diffuse gastrointestinal diseases. In dogs, it has been shown that wall thickness is not sensitive or specific for diagnosis of inflammatory bowel disease1,2. Altered layering patterns may be more significant for evaluation regarding detection of diffuse gastrointestinal disease including inflammatory enteropathies, neoplasia and granulomatous disease.
References:
1. Gaschein L, Kircher P, Stüssi A, et al. Comparison of ultrasonographic findings with clinical activity index (CIBDAI) and diagnosis in dogs with chronic enteropathies. Vet Radiol 2008; 49: 56-64.
2. Penninck DG, Smyers B, Webster CRL, et al. Diagnostic value of ultrasonography in differentiating enteritis from intestinal neoplasia in dogs. Vet Radiol 2003; 44: 570-575.